It is perfect running weather so today I want to discuss a common ailment in runners and other athletes called iliotibial band syndrome or IT Band Syndrome. I like the term syndrome because it appreciates the complexity of this problem. As with many things in the human body, it is not as easy and clearly defined as once thought because if it were, countless runners, cyclists, tennis, football, and soccer players would not still be suffering. So this will be a discussion, not a hard list of what to do for this nagging injury which presents itself as pain on the out side of the lower aspect of the femur and knee.
Interestingly, if you search IT Band pain and treatment you will be provided a list of causes and what to do. Having worked with many individuals over the years with sometimes debilitating and often recurring lateral knee pain, I want to caution you around these standardized lists. Here is a “Top 5 causes of IT Band Syndrome” found on the Internet.
1. Overuse – treatment rest.
2. Tight tissues – treatment foam roller and stretch.
3. Weak Muscles – treatment strengthen.
4. Poor running form – treatment correct it.
5. Inadequate shoes / orthotics – treatment purchase some.
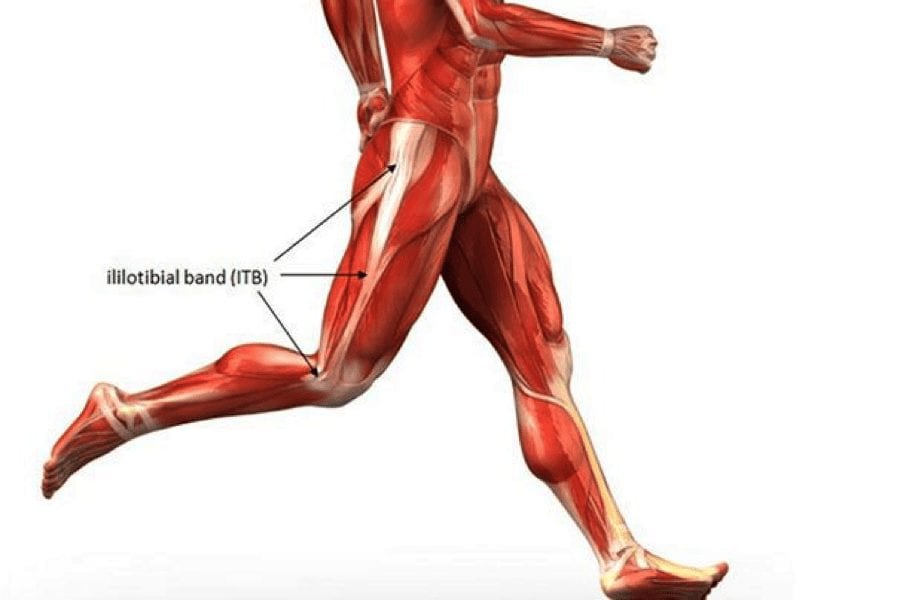
So if it were as simple as this list you should be pain free as long as you rest, foam roll, stretch, strengthen, improve your form and buy a good pair of shoes, but it isn’t this simple. Lets begin with the amazing and complex anatomy that makes up the IT Band. First, it is not simply the tendon of the small but mighty TFL (tensor fascia latae) muscle, but the IT Band also serves as an anchor for the gluteus maximus, medius, minimus, and the vastus lateralis (one of your quadriceps muscles). Second, it is not simply a long tendon connecting muscles from the pelvis to the tibia (lower leg bone), but more accurately a unique tendon – ligament hybrid. Remembering a ligament connects bone to bone, we appreciate the IT Band has discrete deep attachments from the pelvis, along the femur, lateral epicondyle of the tibia, and once integrated with the knee joint capsule itself incorporates the patella. The IT Band is truly a complex, multi-joint, multi-attachment tendon – ligament hybrid controlling a large amount of lower extremity stability especially when on one leg.
I want to spend time on the concepts of “tight tissues” and “weak muscles.” From grade school gym class on, we are taught to stretch tight muscles. But one of the most important things you can do for your body, a recurrent nagging injury, and limiting pain is to understand “why” a tissue is tight. The answer is grounded in the fact that muscle tension is usually a neuromuscular issue not simply a mechanical one. At times a muscle is working too hard, doing too much of a job, and needs to be released to work less and more appropriately. But in this scenario, if you do not also identify accurately what muscle has been off duty or inhibited and re-pattern this motor control you will inevitably see this pattern repeat itself.
There are also times when a muscle is weak / inhibited but at the same time tight and painful. In this case, it is not optimal to stretch or release an already inhibited muscle. So how does one know? There are certainly common patterns that we see in the clinic. Neurokinetic testing and treatment can also assist in systematically identifying the weak / inhibited muscles from the facilitated / over-worked ones and allow the motor control centers in the brain the ability to re-pattern faulty movement. Coupled with closed kinetic chain exercises using the Redcord Neurac Method we can integrate stability between the lower extremities, core, and upper extremities. Helping you finally unravel why these nagging, recurrent, activity limiting pain patterns exist and resolve them.
The take home point about IT Band Syndrome and lateral knee pain is that your pain is most likely a neuromuscular balance issue in the muscles of the hip not a mechanically tight IT Band. The effect of rolling out the entire length of the IT Band itself by direct pressure has little efficacy. Please consider this discussion before torturing yourself and instead find and release the right muscles so the faulty movement pattern can be changed.
Michele Zink Harris, PT, CNP, RAS
Certified Neurac Practitioner / Redcord Active Specialist
Center for Healing and Regenerative Medicine
Reference and further reading at painscience.com.


